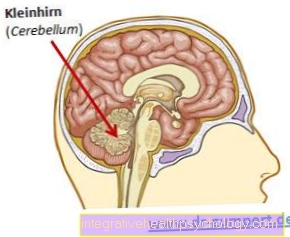
Patellar tip syndrome
Synonyms in a broader sense
Jumper knee, kneecap tip syndrome, patellar apicitis, patellar tendinitis, patellar tendinosis, enthesopathy of the patellar tendon
English: Jumpers knee
definition
It is a chronic, painful, degenerative overuse disease of the kneecap extensor apparatus at the bone / tendon junction of the kneecap tip.

classification
In everyday clinical practice there is usually no classification of the kneecap syndrome.
The most frequently mentioned classification is that of Roels, et al. 1978:
- Grade I: pain after stopping the exercise
- Grade II: Pain at the beginning of the exercise, which disappears again after the warm-up period and reappears after the end.
- Grade III: permanent pain
- Grade IV: patellar tendon rupture (tear of the tendon)
anatomy
The Kneecap (Patella) is as a sesamoid between the upper and Lower leg located on the front of the knee joint. It is part of the knee joint. It has a triangular shape, with the base of this triangle pointing towards the thigh and the tip towards the lower leg. The extensor muscles of the thigh (quadriceps muscles, Quadriceps muscle) ends sinewy at the base of the kneecap. From the tip of the kneecap, the kneecap tendon (patellar tendon) runs to the front of the lower leg (Tibial tuberosity). In this way (quadriceps muscle - quadriceps tendon - kneecap - kneecap tendon - shinbone), the strength development of the thigh extensor muscles is transferred to the lower leg.
The kneecap tendon is particularly exposed to high loads Leap exposed because this results in strong and jerky tensile stress on the tendon. This can overload the tendon tissue.
Appointment with a knee specialist?
I would be happy to advise you!
Who am I?
My name is dr. Nicolas Gumpert. I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The knee joint is one of the joints with the greatest stress.
Therefore, the treatment of the knee joint (e.g. meniscus tear, cartilage damage, cruciate ligament damage, runner's knee, etc.) requires a lot of experience.
I treat a wide variety of knee diseases in a conservative way.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- Lumedis - your orthopedic surgeon
Kaiserstrasse 14
60311 Frankfurt am Main
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at Dr. Nicolas Gumpert
causes

The patellar tip syndrome / jumpers knee is a clinical picture that is caused by overloading the kneecap tendon through repeated, unusual and / or severe tensile loads.
There are both external influencing factors that can cause a patellar tip syndrome / jumpers knee, as well as internal influencing factors.
The activity causing the complaint is one of the external influencing factors. Since maximum tensile stress on the kneecap tendon occurs particularly in jumping sports, sports such as volleyball, basketball, long jump or high jump are frequent triggers for a patellar tip syndrome / jumper knee / jumpers knee. That is why the disease term Springerknie or English. Jumpers knee. The frequency of the load, the intensity of the load and the unusual nature of the load (new sport, beginners) play an important role in the development of a patellar tip syndrome.
But also in cycling, weightlifting, jogging on hard surfaces, tennis, a patellar tip syndrome / jumpers knee is found more often.
The internal influencing factors include:
- the age (mostly patients over 15 years)
- an elevated kneecap (patella alta),
- a history of Osgood-Schlatter disease
For more information on this topic, see: Osgood-Schlatter disease - reduced elasticity of the leg muscles
- as well as a congenital ligament weakness (ligament laxity)
pathology
The structural damage in a jumper's knee affects the tendon / bone transition of the kneecap tendon (patella) at the tip of the kneecap. Microscopic examinations were able to detect significant degenerative (wear-related) changes in the tendon tissue, whereas inflammatory cells were missing. It is therefore a degenerative (wear-related), not an inflammatory disease.
You may also be interested in this topic: Chronic knee pain
Symptoms
Patients with patellar tip syndrome report stress-dependent pain in the area of the tip of the kneecap. Depending on the stage of the disease, the pain can be present at the beginning of the exercise and disappear again after the warm-up phase, while it occurs again in the phase after the exercise. In the advanced stage, the pain remains throughout the load. In very advanced cases, the base of the kneecap hurts not only during exercise but also permanently in everyday life, for example when climbing stairs. Some patients describe a stitch-like pain in certain angular states of the knee joint under load.
Read more on the topic Pain behind the kneecap
The persistent character of the symptoms is typical. Often it is a chronic clinical picture that lasts for many months or years with phases with few symptoms, but recurring symptoms after peak loads.
A patellar tip syndrome / jumpers knee on both sides occurs in 20-30 percent.
Read more too: Patellar tip syndrome symptoms
diagnosis

The medical history (anamnesis) of the patients with jumping sports as hobbies is trend-setting. Frequent jogging on hard surfaces or bodybuilding are also mentioned more often.
The physical examination usually reveals tenderness over the tip of the kneecap. A painful stretching movement of the lower leg against resistance is also typical. Visible redness or swelling are less common signs. Sometimes the knee joint is completely normal, in which case a suspected diagnosis can only be made based on the medical history. Some patients also complain of a feeling of stiffness and pain after prolonged sitting, e.g. after long car journeys.
Imaging procedures
The Sonography (Ultrasound) is a readily available and convenient method for diagnosing a jumper's knee. In order to be able to correctly assess any changes, the healthy opposite side should always be examined. Typical sonographic changes in a jumpers knee are a tendon thickening, an irregularly limited tendon sliding tissue and an inconsistent one Tendon structure.
The MRI scan of the knee does not belong to the routine diagnosis of patellar tip syndrome / jumpers knee, even if it is a suitable procedure.
MRI is important for localizing the area of degeneration if the surgical removal of the changed tendon tissue is due. Furthermore, the quality of the patellar tendon can be assessed better with the MRI of the knee than with sonography.
Further information on this topic is also available at: MRI scan of the knee
The X-ray does not help with patellar tip syndrome / jumpers knee and serves to exclude other diseases.
MRI for patellar tip syndrome
The imaging procedures play an important role in a reliable diagnosis of the patellar tip syndrome.
The focus here is on X-ray image and the Sonography, through which changes in the bones and patellar tendon are clearly visible.
In contrast to them, the Magnetic resonance imaging (MRI) not part of the routine check-ups Jumper’s knee and is therefore rarely used in this case.
The greatest advantage of this imaging method is that it enables the degenerated area to be localized very precisely, which is why it is used in the context of surgical removal of the affected tissue. In addition, the MRI enables differential diagnoses, such as degenerative changes in the Cartilage, for example one Knee osteoarthritis.

I would be happy to advise you!
Who am I?
My name is dr. Nicolas Gumpert. I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The knee joint is one of the joints with the greatest stress.
Therefore, the treatment of the knee joint (e.g. meniscus tear, cartilage damage, cruciate ligament damage, runner's knee, etc.) requires a lot of experience.
I treat a wide variety of knee diseases in a conservative way.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- Lumedis - your orthopedic surgeon
Kaiserstrasse 14
60311 Frankfurt am Main
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at Dr. Nicolas Gumpert
Therapy for a patellar tip syndrome
Taping for patellar tip syndrome
For some years now, taping has increasingly found its way into various areas of medicine. The technology is enjoying increasing popularity, especially in sports medicine and physiotherapy, and is used in the prophylaxis and treatment of a wide variety of diseases.
Depending on the technique used and the tape used, the tape itself (The color of the tape should also play a role) have different effects on the target organ. Although many doctors and physiotherapists swear by taping, it should be emphasized that its effects have not yet been scientifically proven.
Also with the Therapy of patellar tip syndrome Kinesiological tape is widely used. It is used primarily for the prophylaxis of the disease as soon as the first signs of the syndrome appear.
With the so-called Patella tendon tapes and Patella bandages (Jumper knee straps) should be able to avoid long breaks in sport.
In the case of pronounced complaints, however, longer sports leave cannot be avoided, even with tape. Furthermore, taping should enable a faster return to sport after a long break due to the patellar tip syndrome. In both cases it has the function of absorbing tensile forces on the tendon and instead transferring them to the skin on which it was taut.
Shock wave therapy
Patellar tip syndrome is usually treated conservatively, i.e. non-surgically. In addition to various medications, physiotherapeutic and physical measures are used. These include, for example, massages, cold and heat therapy and high-energy extracorporeal shock wave therapy. The target organ, in this case the knee, rests on a plastic cushion filled with water into which sound waves are introduced. These are bundled at the target location, i.e. the affected tissue of the patellar tendon.
Shock wave therapy is used for various diseases, with calcifications and ossifications being the main focus.
A therapy session takes about two to five minutes and can be carried out on an outpatient basis. The cost of extracorporeal shock wave therapy is between 50 and almost 400 euros per session.
Read more on the topic: Shock wave therapy
stretching
In the case of patellar tip syndrome, as well as other consequential damage caused by overuse, the best therapy is good prophylaxis.
Above all, that play for this Warm up before exercising, a slow increase in exertion and sufficiently long breaks between training units play an important role. In addition, however, muscle stretching is also important in order to prevent patellar tip syndrome. Particular attention should be paid to the anterior thigh muscles, especially the Quadriceps femoris muscle (the largest thigh muscle). There are a number of easier options for this Exercises availablewhich should be done especially after training.
In addition to prophylaxis, stretching exercises are also suitable to support the healing of an existing patellar tendon syndrome. For this, the exercises should be carried out at low intensity several times a day for a few minutes. It is important, however, not to overload the tendon.
surgery
In some cases it occurs despite being more consistent Training break and more correct conservative therapy no satisfactory result. In these cases, surgical therapy is the only way to restore
- Sports ability and
- Freedom from complaints.
There are several ways that Patellar tip syndrome to be treated surgically. For one thing, it can Tendon sliding tissue removed in order to remove the offending tissue.
The area around the tendons is cleared so that no disturbing signs of cartilage or inflammation rub against the tendons. In addition, the tendon be released at the tip of the kneecap. This reduces the tension on the tendon Kneecap and thereby improves the symptoms. In some cases, the tendons can be incised lengthways using a laser. This also reduces the tension of the tendons on the kneecap.
All of these procedures can minimally invasive, arthroscopic be performed. In addition, every procedure
- individually, but also in
- combination be applied.
For more information, see: Patellar tip syndrome surgery
Which procedure is used depends on the extent of the tendon change. To be able to determine the surgical procedure, a magnetic resonance scan (MRI) is essential before the operation. If the change is only at the tendon insertion, minimally invasive therapy using arthroscopy is recommended. The tendon can be partially detached and the changed part of the tendon removed.
in case of an stronger or long-distance Tendon damage or partial necrosis of the tendon is common open surgery necessary.
Here the surgeon must individually decide which surgical procedure to use and how much tendon tissue to remove.
There should always be a Post-treatment phase connect. How this looks exactly has to be decided individually. This depends on the findings and the operation performed.
The following phases can be mentioned as an orientation:
- The first 3-5 days After the operation, the knee should be supported by crutches relieved become.
- Then a light one closes physical therapy For approx. 2-6 weeks which slowly through force- and Coordination exercises is intensified.
- Approx. 2- 6 weeks after the operation can be done with a light exercise on the Exercise bike to be started.
- The first easy ones Running exercises can after 4-8 weeks started and then slowly increased individually.
- After approx. 4-8 weeks can first Strength exercises be performed,
- Jump training should only after 6 weeks - 4 months to be started.
The average is full Sports ability depending on the findings 2 to 6 Months to reach.
Healing of a patellar tip syndrome
Since that Patellar tip syndrome is a disease which is due, among other things, to stronger or to longer When stress occurs, the healing depends on one
- consistent therapy and often an initial one
- consistent discharge from.
A single effective therapy for curing the Patellar tip syndrome does not exist. The therapy is made up of various components, which from
- Quiet,
- physiotherapy,
- targeted Strengthening exercises and
- more medicinal or
- physiotherapeutic therapy consists.
forecast
In most cases, conservative therapy is promising if sufficient sports leave is observed. With tape bandages and relieving orthoses as well as a soft shoe sole, recurrences or illnesses can sometimes be avoided.
The success rate after surgical therapy is given in the literature as 70-90% good and very good results. However, the sport-specific return often takes place at a lower sporting level.
If the patellar tip syndrome appears for the first time, the load should be significantly reduced, in some cases even completely absent for a few days. So the im Knee joint heal the resulting inflammation. In some cases, this is initially enough to get rid of symptoms.
Physiotherapy is used in the acute phase warmth- and Refrigeration applications and Ultrasonic worked. Later will be special Stabilization- and Strengthening exercises used to strengthen the tendons of the knee. Also wearing a special one Knee brace can significantly help to reduce pain and promote healing.
In rare cases, the patellar tip syndrome cannot be cured conservatively. Then is one surgery indicated, which leads to full fitness for sport in 70-90% of patients after approx. 2 to 6 months. However, the best therapy is this prophylaxis.
Particularly important here are thorough
- Warm up before sport and detailed
- stretching before and after exercise.
Furthermore, sports activities should not be increased too quickly so that the knee is not overloaded. It is also important to have a sufficient break between sporting activities in order to give the knee enough time to regenerate.
In case of Misalignment of the leg, in the sense of O- or X-legs, can be special Shoe insoles Avoid patellar tip syndrome. All of these prophylactic measures also apply if the patient has a patellar tip syndrome and there are little or no symptoms. This will prevent recurrence of the patellar tip syndrome.
Also improve the individual
- Stretching exercises and the
- bandage the chances of recovery and shorten the healing time.
An exact time period for one Patellar tip syndrome cannot be named. This depends on the extent of the tendon changes and the consistent implementation of adequate therapy and the right exercises.
Complications
The complications of a patellar tip syndrome / jumpers knee include a tear in the kneecap tendon in advanced degeneration or after incorrect cortisone infiltration therapy.
The same complication possibilities apply to surgical therapy as to most surgical interventions:
- Infection, wound healing disorder
- Nerve injuries
- Thrombosis / pulmonary embolism
- Relapse / Remaining Discomfort
- Tendon injury (risk of rupture)