Peroneal tendon syndrome
introduction
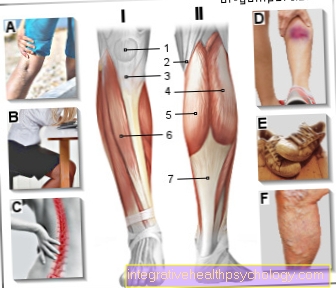
The two tendons of the short and long fibula muscles (old name: Musculus peroneus longus et brevis; newer name: Musculus fibulais longus et brevis) denotes the approach and thus the connection between the Foot bones and the Musculature of the lower leg on both sides of the calf.
The long fibula originates from the upper end of the fibula and runs towards the outside of the fibula footto then pull behind the outside ankle and under the foot and along the inside of the first Metatarsal to apply.
The short fibula takes a similar course, but is, according to its name, shorter and therefore originates a little further down on the fibula to later attach to the outer edge of the fifth metatarsal.

The function of both muscles is to extend the foot downwards (Plantar flexion), spreading the foot or moving the foot away from the center of the body and lifting the outer edge of the foot or bending the foot axis inwards (Pronation). Both muscles also stabilize the foot while walking.
Both tendons of the fibula muscles run in a bony groove that is covered by a sheath of connective tissue (Retinaculum) is surrounded. This guide channel enables the tendon to sit securely or slide, as well as optimal power transmission to the foot.
If the fibula muscles are chronically improper or overloaded, this can lead to reactive inflammation of one or both peroneal tendons or to the so-called peroneal tendon syndrome, which is sometimes characterized by severe pain and discomfort during certain foot movements.
root cause
The cause of the Inflammation of tendons (Tendovaginitis; Tendinosis) is usually in the permanent overloadin which it becomes a response to the chronic friction of the tendon in its bony abutment Inflammation of the tendons themselves and / or that enveloping the tendons Tendon sheaths comes. On the one hand, the muscles or the muscle-tendon attachments are overloaded sudden, very strenuous movements without sufficient, previous Muscle warming, but also through incorrect or unfamiliar training with a too rapid increase in load over the course. It can also be permanent Improper loading by anatomical misalignments also cause tendinitis.
Wrong ones especially in the area of the foot Footwear and Misaligned feetlike the O-shaped bending of the foot outwards (Varus position of the ankle) to Peroneal tendonitis to lead.
But possibly also anatomical bone variants permanent irritation of the Peroneal tendons lead, for example with a Peroneal tubercle (bony protrusion in the area of the outer ankle) or one Bone spur may be the case on the fibula.
In some cases, the inflammation of the peroneal tendons can also be due to an infection or as part of a inflammatory rheumatism be conditional.
Please also read our article on this Tendonitis on the ankle or Tendonitis on the sole of the foot.
Appointment with ?

I would be happy to advise you!
Who am I?
My name is dr. Nicolas Gumpert. I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
Athletes (joggers, soccer players, etc.) are particularly often affected by diseases of the foot. In some cases, the cause of the foot discomfort cannot be identified at first.
Therefore, the treatment of the foot (e.g. Achilles tendonitis, heel spurs, etc.) requires a lot of experience.
I focus on a wide variety of foot diseases.
The aim of every treatment is treatment without surgery with a complete recovery of performance.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- Lumedis - your orthopedic surgeon
Kaiserstrasse 14
60311 Frankfurt am Main
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at Dr. Nicolas Gumpert
Symptoms
The peroneal tendon syndrome is characterized by pain in the area of the outer ankle, which is particularly pronounced when the ankle is subjected to stress (especially when lifting the inside of the foot) but can sometimes also occur at rest. A so-called "start-up pain" is also often reported, which mainly occurs in the morning after getting up or after sitting or lying down for a long time. This pain can be accompanied in part by swelling in the area of the outer ankle as well as reddening and warming of the skin in this area.
In some cases, a painful thickening and hardening of the peroneal tendons behind the outer ankle can be felt and a muscular weakness can be felt when attempting to lift the outer side of the foot. The latter symptom leads to a slightly limping gait pattern in the affected patient.
If the inflammatory process spreads to the sural nerve, which accompanies the peroneal muscles and is responsible for the sensitive innervation of the outside of the foot and heel, sensory disturbances and / or a burning sensation in the skin of the outer foot can also occur.
Read more on the topic: Fibula pain
diagnosis
The diagnosis of peroneal tendon syndrome can usually be based on the anamnese of the patient if this is of the characteristic pain reported in the area of the outer ankle and a previous mechanical stress on the foot.
When the patient is physically examined, this usually comes to mind Arches foot and a forefoot position that tends inward when standing straight and is often accompanied by an O-shaped deviating ankle axis.
If the medical history and physical examination are inconclusive, you can imaging procedures support the diagnosis. Different imaging options come into question, depending on the question and which differential diagnoses are to be excluded.
The Ultrasound examination (Sonography) provides the method of choice Assessment of the tendons because this is an inexpensive, simple and time-saving method for the detection of inflammations and tears in the tendons or tendon sheaths.
The Magnetic resonance imaging (MRI) serves to expand or supplement the ultrasound diagnostics and enables an even more precise assessment of inflammatory processes and tendon tears. Also typical of peroneal tendonitis edema in the area of the outer ankle can be shown more clearly in the MRI.
The classic X-ray of the foot primarily provides information about pathologies on the bony foot skeleton (Fractures), about changes in the ankle (arthritis) as well as possible Misaligned feet (Hollow or flat foot).
In addition, a Blood collection be useful to infection and inflammatory rheumatic diseases based on Inflammation parameters to be able to exclude or prove in the laboratory.
therapy

The first treatment for peroneal tendon syndrome is usually one conservative attempt, which is primarily a discharge of the tendon to allow the inflammation to subside.
This can be achieved through a Splint, Bandaging or taping the ankle, creating a temporary one Immobilization is effected in the ankle. The overloading movements or the previously exercised activity should also be reduced or even stopped for a few weeks, especially activities with rapid changes of direction.
That too Cool with an ice pack of the outer ankle at an interval of 10-20 minutes, one can Symptom relief achieve.
Medicinal is a parallel treatment with pain relievers and anti-inflammatory drugs (for example Ibuprofen or Diclofenac), which can contain the inflammation in the peroneal tendons. In some cases it can also be a direct injection Cortisone narcotic mixture in the immediate area of the inflamed tendons be helpful to a local Anti-inflammatory and pain relief to reach.
The cause of the inflammation is one bacterial infection, sometimes becomes a Antibiotic therapy initiated.
In addition, seeking out is one Physiotherapists meaningful with the targeted Strengthening exercises the lower leg muscles can be carried out to compensate for any existing muscular imbalances and to strengthen the fibula muscles.
If there are misaligned feet, compensatory measures can also be used Footbed insoles lead to a significant relief of the peroneal tendons, so that, for example, an insert with a cut-out area under the first metatarsal bone in patients with Arches foot correct the misalignment.
If conservative therapy fails, the inflammatory process is very strong and advanced, or it may be lying anatomical bone variants such as If, for example, a prominent peroneal tubercle or a bone spur is found, surgical treatment can be a good alternative.
The Surgical method depends largely on the goal pursued and the underlying cause of the peroneal tendon syndrome. One is possible Cleansing the inflamed tendons (Debridement, synovectomy), a smoothing of the tendons or their troughs, a repair of tendon tears or tears, a restoration of the peroneal retinaculum or a resection of the peroneal tubercle.
In the case of massive foot deformities, even a Change in the rearfoot bone arrangement (lateralizing calcaneus osteotomy) or one Stabilization of the ankle ligaments be the only therapy to correct the problem.