Impingement syndrome of the shoulder - physiotherapeutic assessment
Note
You are in the subtopic Physiotherapy for impingement syndrome.
You can get to the start page for this topic at Physiotherapy for impingement syndrome.
You can find the medical-orthopedic part under our topic Impingement Syndrome, written by Dr. Nicolas Gumpert.
Appointment with a shoulder specialist

I would be happy to advise you!
Who am I?
My name is Carmen Heinz. I am a specialist in orthopedics and trauma surgery in the specialist team of .
The shoulder joint is one of the most complicated joints in the human body.
The treatment of the shoulder (rotator cuff, impingement syndrome, calcified shoulder (tendinosis calcarea, biceps tendon, etc.) therefore requires a lot of experience.
I treat a wide variety of shoulder diseases in a conservative way.
The aim of any therapy is treatment with full recovery without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- Lumedis - your orthopedic surgeon
Kaiserstrasse 14
60311 Frankfurt am Main
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
You can find more information about myself at Carmen Heinz.
Anamnesis - taking a history
Before the physiotherapist can come up with an effective treatment concept based on the causes of the pain, a detailed one is required anamnese = Establishing a medical history is essential to distinguish between primary and secondary impingement.
Most important questions:
- How long have the symptoms persisted?
- How bad is the pain? Visual analog scale- Pain scale from 1-10
- What movements or loads trigger the pain, what relieves?
- How strong is the irritability, which stress, minor or severe, trigger the pain?
- “Everyday bad posture?”, Constantly recurring movement sequences in your job?
-
Are there complaints in the cervical or thoracic vertebrae at rest or when moving and exercising?
- Accompanying symptoms such as tingling or weakening of sensitivity in the arm or hand?
- Relationship between shoulder symptoms and complaints in the Gastrointestinal tract or the bilee.g. after eating?
Manual examination
1. Palpation = tactile examination always in side comparison
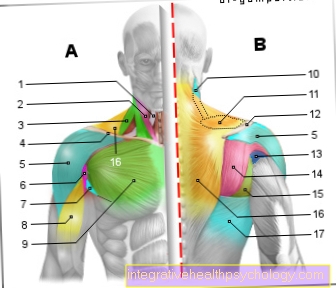
- Swelling of the Rotator cuff tendons (Torsion and splay muscles of the Shoulder joint) palpable over the bony attachment, combined with resistance tests of the affected Musculature
- Position of the shoulder joint head forwards (subluxation - indication of instability) or shifted upwards (indication of entrapment under the shoulder roof)
- Normal 0 21 false false false DE X-NONE X-NONE MicrosoftInternetExplorer4
-
Standing out of the shoulder blade in a side-by-side comparison?
- High muscle tension in the shoulder girdle muscles and the presence of trigger points indicate a muscular imbalance
- Tenderness of the nerve exit points at the Cervical spine indicate involvement of the cervical spine or the Nervous system
- Palpation of the scars in the abdomen
2. Functional investigation
- Direction of movement to limit the painful arch, too early movement of the shoulder blade (changed rhythm of movement between Shoulder joint and shoulder blade) indicates instability of the shoulder joint
- At the front drawer phenomenon The practitioner examines the sliding movement of the shoulder head forwards and backwards in the shoulder joint = instability test, possibly there is a laxity (loosening, overstretching) of the anterior capsule parts and a shortening of the posterior parts of the capsule
- Sulcus sign: increased sliding movement of the shoulder joint head downwards compared to the shoulder blade
-
Test for inflammation of the bursa: Passive spreading movement of the arm under tension
- Passive movement test of the shoulder joint by splaying the arm under different rotational positions to find out whether the pain is increased or relieved
- Manual resistance tests for the shoulder muscles, releasing the Spreading and external rotation of the shoulder joint greatest pain
- Strength tests of the shoulder joint and shoulder blade muscles
- Testing of muscle elasticity, test for muscle shortening
- Active and passive movement tests of the cervical and thoracic spine
- The patient holds the arm in the symptom-triggering position, the therapist moves the cervical spine to the side, in a rotating position or with pressure and checks whether the pain is intensified or the arm is relieved
- If the rib joints are blocked, deep breathing causes shoulder pain
- Nerve stretching of the upper extremity triggers shoulder pain, nerve proximity brings pain relief in the shoulder and thus provides evidence of involvement of the cervical spine and the nervous system
- Organ involvement must be considered if there is pressure on the therapist's hand Stomach, bile or liver When the organs are released, the shoulder symptoms intensify (the patient holds the arm in the symptom-triggering position during the test)
3. Differentiation of the primary impingement syndrome
- Supraspinatus tendon: Empty can test, lifting and spreading movement of the arm against resistance during internal rotation in the shoulder and forearm (thumbs down)
- Infraspinatus tendon: painful resistance test during external rotation of the shoulder joint
- Biceps tendon: full can test, lifting and spreading movement of the arm against resistance during external rotation in the shoulder and forearm (thumbs up)
- In addition: painful resistance test against elbow flexion and internal rotation, if “full and empty can” test both positive, conclusions can be drawn about a rotator cuff injury
- Hawkins test: provocation of the known pain by passive internal rotation of the shoulder joint from a 90 ° raised position
- Neer's test: Pain provocation through maximum lifting movement of the shoulder joint with the shoulder blade passively fixed
- Stability test of the shoulder blade (SAT, SRT)
- Test for shoulder joint instability: Examination of the sliding movement of the shoulder head forwards and backwards; the sliding movement forwards is often increased = this instability can force a muscular impingement
- Test for bursitis: Passive relief of the bursa under tension with passive splaying motion brings pain relief
- Foreshortening tests of the pectoralis major and shoulder blade lifter
On the basis of all the test results, the physiotherapist creates a hypothesis, whereby there can be several causes that trigger pain. A treatment plan is drawn up and trial treatments are carried out. Through regular "retests" (repeat findings after treatment) the physiotherapist can identify which treatment techniques are most effective and possibly change the treatment plan accordingly.